Did you know that haemorrhoids are so common, that they will cause symptoms in at least 1 in 3 people? Read on for more, and remember that you are not alone!
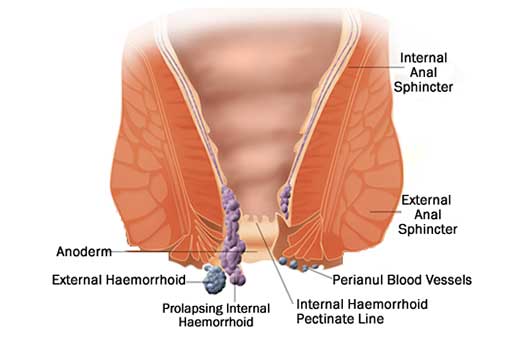
Haemorrhoids (or ‘piles’) are the enlargement of a small network of blood vessels in the anal canal. They are very common – affecting between 25-50% of the population. They do have a normal function, and help to occupy space in the anal canal, and contribute to anal tone – this helps prevent soiling, leakage, and the involuntary loss of wind.
Haemorrhoids can lose their attachement to the wall of the anal canal, allowing them to slide, enlarge and prolapse. As haemorrhoids enlarge, they become fragile and can cause bleeding – this is usually small volume, bright red, and fresh blood on the toilet paper, in the bowl, or on the outside of the stool. Occasionally, blood will leak into the underpants, particularly with passing wind. Bleeding from haemorrhoids can be major, but this is less common. Bleeding after anal sex may be due to trauma or tears, or aggravation of underlying haemorrhoids.
Whilst haemorrhoids are benign and rarely dangerous, it is important to exclude more worrying causes of rectal bleeding. This includes rectal polyps or rectal cancer, and unfortunately in young people, rectal cancer is increasing in incidence. We cannot presume that bleeding is due to haemorrhoids. Bleeding is not normal, and you should see your doctor – don’t die of embarassment.
Haemorrhoids can also prolapse to the outside, with defecation, passing wind or even physical activities. These can irritated, uncomfortable, and they can cause soiling, mucous and ‘skid marks’. Prolapsed haemorrhoids can make cleaning difficult, and the combination of leakage and difficulty with cleaning can cause itch and irritation of the skin around the anus. If haemorrhoids get really stuck on the outside, they can become very swollen and painful – this is called “acute thrombosed prolapsed haemorrhoids”.
Unless they do become stuck, haemorrhoids aren’t typically painful – and this is a common misconception. Pain associated with defecation is not usually haemorrhoids, and we need to consider other diagnoses such as an anal fissure, fistula, infection or cancer.
There are multiple options for treating haemorrhoids – and there are even painless options!
Dr Morris is an enthusiast for avoiding painful haemorrhoid treatments where possible, and has a range of minimally invasive options that will be discussed if suitable, for you. It is important that your surgeon considers your function, and your goals, for example, if bottoming is important to you, then this should be considered, addressed, and please feel comfortable raising it – Dr Morris talks about this all day!
Please see some of these options below, and in the “Procedures” tab, but your possible options will be carefully discussed in your consultation.