Anal fissures can be excruciatingly painful, and can make defecation a harrowing and fearful experience. But you don’t need to continue to suffer – anal fissures are common, and we have options for treatment.
An anal fissure is a tear in the lining of the anal canal, just inside or at the anus. It usually causes a sharp, tearing sensation when having a bowel motion – it feels like passing glass. The underlying anal sphincter then goes into spasm, which causes a deeper, often severe pressure or throbbing sensation which can last minutes to hours. This pain can also be brought on with sitting or driving, and can be more debilitating than the painful bowel motion itself.
The anal spasm is thought to prevent blood flow to the healing wound, thus the anal fissure may not heal on its own, becoming stuck in an ongoing cycle of pain and non-healing.
An acute fissure (present for less than 2-6 weeks) may improve with increased fluid and fibre intake, warm baths, and stool softeners. Whilst over the counter options exist, only topical Rectogesic or Diltiazem address the spasm to hopefully allow healing.
A fissure that is present longer than six weeks, or one that recurs, is considered a ‘chronic anal fissure’. This will not usually respond to topical creams. Treatment for a chronic fissure is tailored to your individual circumstances and treatment goals. Options include the injection of botox or a small cut in the sphincter (called a lateral internal sphincterotomy) to relieve the painful pressure and allow healing.
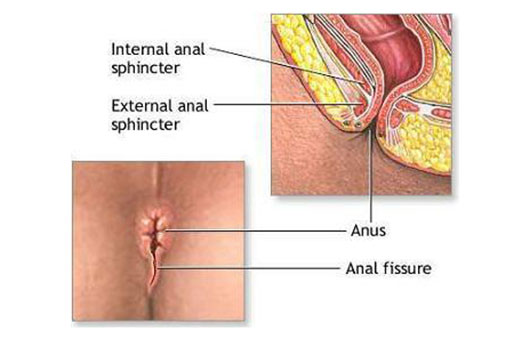
Anal fissure diagram
The tear results from an initial trauma - and then gets stuck in a cycle of repeated tearing and non-healing.
An anal fissure is a tear in the lining of the anal canal, which may occur following the passage of a hard stool, an episode of diarrhoea, or trauma following anal sex. (Embarassed about this? Guess what… people have anal sex, its no secret… we have heard it hundreds of times. We are here to help).
This can result in often severe pain with the passage of stool – considered by many some of the worst pain imaginable! The pain is typically ‘sharp’, ‘tearing’, ‘like passing glass’ or can be a deep-seated throbbing pain. The pain may last minutes to hours. There may be an associated small amount of bright-red bleeding seen on the toilet paper.
The tear results from an initial trauma, which may be due to the passage of a hard stool, or the precipitating event may not be recognised. The pain results in muscle spasm, which exacerbates the pain. Furthermore, the muscle spasm impairs blood flow to the fissure, which in turn prevents healing. This allows a continuous cycle of tearing, pain, muscle spasm, lack of blood flow, poor healing and further tearing.
Treatment is aimed to break the cycle. Initial treatment may be topical creams to relax the muscle sphincter (e.g. topical GTN (Rectogesic) or topical calcium channel blockers (eg diltiazem). Warm baths may help lower the muscle pain and provide symptomatic relief or surgery may be required for anal fissures that persist.
What happens when an anal fissure persists?
An acute fissure is unlikely to heal on its own if the symptoms have persisted after six weeks, and at this stage we call it a chronic anal fissure. At this stage, a more definitive relaxation of the sphincter muscle is required. This can be through an injection of botox to the sphincter, or with a minor surgical technique known as a sphincterotomy.
The precise course of treatment needs to be tailored to the individual patient.
There is much fear and misinformation around anal fissure surgery. In times past, incontinence rates were high – treatment was very brutal, such as an “8 finger stretch”. We don’t do this anymore. Treatments are much safer, and the preservation of continence is paramount. Botox is well tolerated, low risk, and any adverse effects are temporary. Even definitive surgery is tailored to your risks and lifestyle, and any potential impact on your continence should be discussed and minimised.
Less commonly, anal fissures may be associated with other diseases (such as an atypical infection, HIV, or Crohn’s disease, an inflammatory condition), or the symptoms may reflect an alternative diagnosis. If the symptoms fail to respond to a single short-course of treatment (e.g. topical creams), then investigation is usually warranted. Particular warning symptoms raise alarms that we may not be dealing with an anal fissure – these include pain NOT associated with defecation, bleeding mixed in with the stool, new incontinence, a recent change in bowel habits, or a personal or family history of colonic polyps, bowel cancer or inflammatory bowel disease.